A Look Back at the Influenza Epidemic in Siam 101 Years Ago

Over 101 years ago, Thailand faced an outbreak of influenza. The Facebook page of Kamnoon Sidhisamarn revealed historical information about the influenza outbreak in Siam during 1918 to 1919, or 100 years ago, which was published in the Royal Gazette on November 3, 1918, Volume 35, Pages 1855 - 1856, and on July 27, 1919, Volume 36, Pages 1193 - 1202, based on research by Professor Kritsada Boonyasamit, as shared by Professor Suda Wisarutpichai.
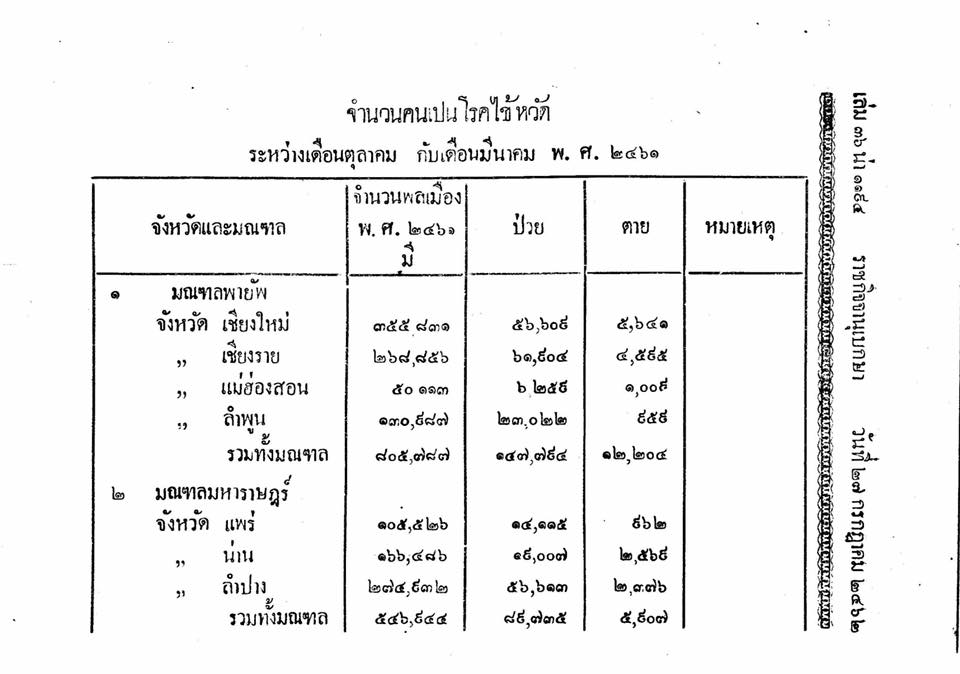
Upon reading the report summarized in the Royal Gazette on July 27, 1919 Volume 36, Pages 1193 - 1202, particularly on page 1202, it reveals that the total number of cases in 17 provinces, excluding Bangkok, was 2,317,662, which is about 1 in 4 of the total population in those provinces, with 80,223 deaths.
At that time, the Siamese government took full responsibility, sending doctors to every province, as noted in the Royal Gazette on November 3, 1918, Volume 35, Pages 1855 - 1856.
"100 years later, today, Thailand's medical and public health systems have improved significantly, effectively managing the situation through the cooperation of the entire population and the government's appropriate measures at each stage. We, the Thai people, will surely overcome the COVID-19 pandemic soon."


Recently, Thailand has faced several significant epidemic challenges. Today, I will highlight two important events:
History of Emerging Diseases: ‘SARS’ - The Global Pandemic
“SARS” was dubbed the global pandemic, originating in China, from Guangdong to Jilin, Hebei, Shanxi, Tianjin, and Inner Mongolia. The World Health Organization issued a global alert about the dangers of SARS on March 12, 2003, followed by a warning from the U.S. Centers for Disease Control and Prevention. At that time, the disease had spread to Toronto, Ottawa, San Francisco, Ulaanbaatar, Manila, Singapore, Taiwan, Hanoi, and Hong Kong.
According to the book “Global Epidemics, Volume 4” by Professor Emeritus Dr. Prasert Thongjaroen, it discusses the origins of SARS and the period of its outbreak interestingly.
“The news of the SARS outbreak did not start from any country's health ministry or the World Health Organization, but began in a 'chat room' on the evening of February 9, 2003. Catherine Strommen, a primary school teacher in Fremont, California, was chatting in a 'Teacher Net' chat room, as she usually did, exchanging knowledge and experiences with fellow teachers. A man named 'Ben' from China entered the chat.”
“Ben” recounted that he was from Guangdong and was unaware of any strange illness in his hometown. People who seemed fine suddenly developed flu-like symptoms, and within a day or two, they were struggling to breathe and died. A friend of Ben's worked in a hospital, and that friend's mother also died. Anyone who entered the hospital never returned, dying in narrow coffins. Ben tried to reach out to see if anyone outside China knew about this and could help him.
Shortly after, an internet report from “ProMed” on March 12 cited the WHO Weekly Epidemiological Record, stating that there was an outbreak of pneumonia from Guangdong. It noted that since mid-November 2002, there had been an unexpected occurrence of atypical pneumonia in Guangdong, China, with 305 cases and 5 deaths reported by February 2003. Autopsies revealed that some cases (2) were caused by a pathogen known as Chlamydia pneumoniae, but Chinese authorities remained silent and did not inform anyone until the disease became public knowledge.
The first patient occurred in the city of Shunde, Foshan, Guangdong Province in November 2002. This patient was a farmer who was treated at the First People’s Hospital of Foshan and died shortly after admission, but no clear diagnosis was made for the cause of death. Chinese officials not only failed to inform anyone but also tried to suppress the news, limiting media coverage. The emergence of this new disease was not revealed until February of the following year, leading to widespread criticism of the Chinese government from the global community, which later apologized for the delay.
“The SARS virus spread from China to Hong Kong, likely originating from Professor Liu Jianlun, a nephrologist from Songshan University, who traveled to Hong Kong and stayed at the Metropole Hotel in Mong Kok, Kowloon, where he ultimately died from the disease. Sixteen guests on the same floor contracted the virus and it spread to nearly a thousand people.”
The term SARS, which stands for Severe Acute Respiratory Syndrome, is a newly coined term that had never appeared before. The first reported case of this disease was in March 2003, from Hanoi, Vietnam, involving a businessman named Johnny Chen, who traveled from the U.S. to do business in Guangdong and then continued to Hanoi via Hong Kong, staying at the Metropole Hotel before proceeding with his business in Vietnam. Johnny began to show flu-like symptoms and sought treatment at the French Hospital in Hanoi, a popular choice among Westerners. His condition worsened, requiring a ventilator, and he was eventually sent to Hong Kong, where he died. The name of the disease originated at this point before he passed away in Hong Kong.
“Johnny” spread the SARS virus at the French Hospital in Hanoi, leading to at least 22 staff members dying from the disease. Before their deaths, these 22 individuals also spread the virus widely in the Hanoi community.
The pathogen causing the deadly flu is the Corona virus, which can be isolated from the tissues of several patients and cultured from the nose and throat. When tested for immune response, it was found that the molecular biology tests indicated characteristics similar to the original strain of the Corona virus, but it was a new strain, hence it was called SARS Coronavirus or Scorona virus.
SARS has an incubation period of approximately 2-7 days from infection to symptom onset, although some reports indicate it may take up to 10 days. For Thailand, the Bureau of Epidemiology, Ministry of Public Health, allows a 14-day observation period for symptoms to appear. About 10-20% of patients experience severe symptoms requiring ventilators, with a mortality rate of 6-15%, often resulting in pneumonia and death. Symptoms may be mild at first but are not significantly different from flu symptoms.
As for the treatment of the deadly flu, the latest information indicates that there is no effective treatment plan. Most treatments are for pneumonia of unknown cause, consisting of supportive care, with some receiving antibiotics, antiviral medications like oseltamivir or ribavirin, and some receiving steroids, but the results remain ambiguous.
Lessons from the 2009 Influenza Pandemic in Thailand
Another case is the 2009 Influenza Pandemic, which in March 2009, Mexico reported an unusual increase in patients with flu-like symptoms, initially mistaken for seasonal flu, until reports of deaths from unknown pneumonia emerged. By April, the U.S. Centers for Disease Control and Prevention announced the discovery of a new strain of influenza in California, identified as type A, which could not be differentiated by standard methods.
In May of the same year, the first two Thai patients were reported after returning from Mexico, followed by reports of new strain influenza cases in the country. The new strain of influenza spread rapidly, especially in schools, and by September, the severity of the outbreak decreased, with a total of 165 reported deaths by the end of September. However, from this situation, Thailand learned lessons in controlling the new strain of influenza in 2009 as well.
Looking back at the outbreak of the new strain of influenza in 2009, which spread rapidly worldwide within two months, Thailand experienced a rapid domestic outbreak in June 2009, primarily driven by elementary and secondary school students. The outbreak began in Bangkok and the surrounding areas, spreading to all provinces. Moreover, students transmitted the outbreak to their families, leading to parents getting infected and spreading the virus to their workplaces and communities, resulting in approximately 10 million infections by the end of 2009.
Overall, Thailand managed to control this outbreak, reducing deaths by about half, or approximately 500, and slowing the spread through multiple waves with strategies to reduce illness and mortality, including staying home to recover, halting activities in crowded places, promoting handwashing, cleaning personal items, wearing masks, and screening patients to prevent them from participating in community activities. Rapid diagnosis and treatment with antiviral medications, as well as vaccination for high-risk groups, were also implemented.
This outbreak provided important lessons in emergency and crisis management that Thailand must develop, particularly in managing epidemic control, including communication issues to practitioners at the provincial and district levels to ensure comprehensive access to information.
At the same time, communication problems with society during crises created confusion and uncertainty. However, after changing daily press conferences to weekly ones and involving academics or experts from the World Health Organization, public panic was significantly reduced.
Importantly, the outbreak of the new strain of influenza in 2009 led to opportunities for development in various public health areas, such as disease surveillance systems. In the past, influenza surveillance only included reports of illness and death. The outbreak of the new strain of influenza prompted the development and strengthening of disease surveillance systems, including monitoring patients with flu-like symptoms, tracking the detection rate of influenza in specific areas, monitoring outbreak news, and monitoring illness and death, as well as post-vaccination symptom surveillance.
Laboratory development from this outbreak enabled various units to enhance their capabilities to conduct PCR testing, expanding testing to all 14 medical science centers, Bamrasnaradura Institute, various medical faculties, and some private hospitals and laboratories.
Vaccine development was supported by the World Health Organization, encouraging the Government Pharmaceutical Organization of Thailand to develop a prototype factory that meets standards and to research and develop the production of live attenuated influenza vaccines, as well as establish industrial-level factories for producing inactivated influenza vaccines, ensuring sufficient supply for domestic needs.
Additionally, the development of epidemiological networks for disease surveillance and investigation, laboratory networks for diagnosis, and treatment networks, along with continuous public education campaigns, were established.
"It can be seen that the epidemics that occurred 100 years ago up to the present have created pathways for the development of medicine in a positive direction to control, solve problems, and care for the population in emergency situations, just as today, when most people are facing the COVID-19 virus. I believe that cooperation in care and prevention, if achieved through collaboration from all sectors, with the public maintaining cleanliness and adhering to government mandates such as 'Stay Home, Stop the Spread for the Nation,' will significantly reduce the number of infections."
“Infectious diseases will not spread if contact is reduced.”
References:
Professor Emeritus Dr. Prasert Thongjaroen, “Global Epidemics, Volume 4,” 2009.
Lessons from the Control of the New Strain of Influenza 2009 in Thailand by Dr. Kamnoon Uengchusak.
Source: Dr. Suwit Wibulpolprasert (Editor), Thai Public Health 2008-2010, Policy and Strategy Bureau, Ministry of Public Health, 2011.